A conference for open-source enthusiasts is kicking off today in Houston.Organizers are billing FOSSHealth, which stands for Free and Open Source Software in Healthcare, as an “unconference” for people who want to see the latest open-source projects available. Open-source initiatives by Medsphere Systems Corp., Misys, Sun Microsystems and WorldVistA are expected to be presented, according to the agenda.
Fred Trotter, a programmer and co-founder of the Liberty Medical Software Foundation, will introduce the conference. The not-for-profit foundation promotes the use of open-source health information technology. Bill Vass, president and chief operating officer of Sun Microsystems Federal—a Sun Microsystems subsidiary that manages federal government business—and chief technology officer for global accounts and industries at Sun Microsystems, will deliver a keynote about the company's efforts in the project aimed at tying health systems into the national health information networking using free software called Connect.
Maybe not. Look at sponsoring companies, then compare to roster of firms with reps on working groups at CCHIT.
However, if you're interested in data portability/standards in healthcare, keep an eye on FOSSHealth.
31.7.09
The CCHIT Open-Source Certification Body Alternative We've All Been Waiting For?
29.7.09
..."The Language of Health Ought to be Inclusionary"...
Inuktitut can help communicate important unifying concepts in healthcare that may elude us in English. I was reminded of the bonding power of Inuktitut by our new kisaut ("anchor" or "oneness") fellow, Jen McCabe Gorman. Inuktitut is a language of inclusiveness. English can be divisive. Inuktitut is an aggregating language - pronouns, verb tense, and emotional cadence get mixed together to form one block or phrase. And the language of health ought to be inclusionary.
From Neil Seeman's essay: "How Do You Say "Health" in Inuktitut?" Longwoods Publishing
If you're working on NLP for healthcare, semantic web technologies, or creating new ontologies for PHRs, please consider 'meaningful use' of inclusionary language a vital design element.
PHR Business Model Cheat Sheet, and Why I'm So Hung Up on Infoviz
| If you're in the market of trying to help consumers improve overall health and wellness, one microchoice at a time, then you are armpit-deep in the data market, my friend. Personal Health Records (PHRs) providers are, in essence, next-gen health data companies. Yes, this is a vast oversimplification, due to the 'sensitive' nature and uniquely weighted values of health data. Not having info about the cheapest used bicycle for your next Holland tulip tour may not be a life or death issue, while knowing about the latest treatment modality for your type of pancreatic cancer may be. But for the sake of argument, and injecting a healthy dose of common sense before it's legislated right out of the personal health data market, let's take the 'PHR providers = data companies' at face value (at least for now). If you're still reading, and agree to consider the data company angle, this means that once you understand the challenges/opportunities facing next-gen data companies, you can easily extrapolate clear, useful information about what's coming down the pipe, at a macro level, for personal health information (PHI) platforms, and all without gazing into a crystal ball or opening a vein under a full moon. Consider it my gift to you, without making you sign a patient-centric info manifesto in blood. In all seriousness, this isn't fortune-telling, but we've been treating healthcare futurism like it's an occult art. Done right, it's not. Let's take a critical look at business models, current provisions, and market opportunities for data companies, from 30,000 feet. If you're a next-gen, '3.0' data company, you've essentially got 4 business model choices. You can: 1. store data - charge $ somehow 2. sell data - charge $ somehow 3. get consumers to pay you to A. store data (number 1) or B. NOT sell data (number 2) 4. analyze data - charge $ somehow Current PHR companies, including the "Big 2" Google Health and Microsoft HealthVault (which are really just data companies), are organized loosely as rather inefficient answers to business model option 1. A developer friend working on an interesting problem wading through a pedestrian infrastructure solution today made a remark about 'dirty code.' Looking at PHRs as a business model solution to 'storing data,' option 1 above, is a model, but it's an ugly-duckling one. It's necessary, but it's dirty code that doesn't illuminate elegant solutions in a simple, Ruby-on-Rails type manner. But that ain't all bad...let's take a look at what will happen next. Next, PHR companies will pull a Twitter, and figure out their largest asset is all that PHI. When PHR providers figure out they can sell all that chewy personal data (even if anonymized, a la Patients Like Me), they're going to go after business model option 2 - sell data. Now, if you're following, right about now the 'aha! Holy sh*^!' lightbulb should pop on just above your frontal lobe and hover...Option 3 is the holy grail of PHRs. Everyone (or at least a goodly chunk of govt, insurers, and HC reform types) want to get consumers engaged in their healthcare so we cost the system less overall (supposedly anyway). But how to do this? We have to get people interacting with personal health data and 'taking ownership' - which means we want them to give us their data so we can figure out how to make money in one of the ways above. The smart money is on designing for business model option number 3; building something so beautiful and intuitive in terms of visualization and data presentation, that consumers will actually pay either to use it or to restrict how we use it. Add a little functionality, a little meaningful-use, interoperability juice and you've got the fountain of youth, or as near as HIT is going to get us. But the really, really, really, really smart money (and VCs your saliva glands should be in overdrive right about now) is on the sort of rare organization that designs for number 3 but builds for number 4-from Day 1. Without building in a backend analytics platform so crisp you could bounce a quarterweight reduction of the national, bloated BMI off of it, we won't reach critical mass. It is exceedingly well designed analytics that will accelerate us, cold fusion style, towards critical mass adoption of a consumer health platform, guided by super elegant infoviz design that makes string theory look like kloogey code. So what is the penultimate, next-gen PHR model? Look for business model option 3, backend stealth style data analysis integration, and KISS infoviz. Only with all these elements in place will we be able to trick, ahem, talk, consumers into the kind of healthcare decision-making process necessary to change your mind, my mind, and Grandma Nagy's mind away from serving that protean-continent sized slice of pie for desert. You can't manage what you can't measure, and we're doing a pretty good job of mangling even option 1, or storing health data effectively enough to charge w/out a common spec. I don't need to tote at Tarot deck to see the Reaper and the Fool having a field day with our sector. I also, however, don't need runes to read that a bright future is possible with one strange turn of the cards. Jen S. McCabe @jensmccabe CEO/Founder: Contagion HealthCoFounder: NextHealth (NL) Consulting/Chief Patient Advocate (social media): LinkedIn: Jen McCabe iPhone: 301.904.5136 |
Only 27% of Us Think Congress Has "Good Understanding" of Health Care Issues
Dr. G. from Leonardtown, Maryland writes:
I think the question should have been: “How confident are you that Congress has your best interest at heart when it comes to this health care issue?” Answer: Not at all. It seems Congress is intoxicated by lobbyists and their deep pockets and we’re just a piece of chewing gum stuck to the bottom of their expensive shoes.
First comment - a doc from my old hometown (Leonardtown, MD). Excellent to see some political-mindedness, even if it is critical of lobbyists, arising from SoMD.
From the Cafferty File: "Tell Jack how you really feel"
Blog Archive - "How confident are you that Congress understands health care issue?" « - Blogs from CNN.com
28.7.09
Contagion: It's a Beautiful Thing...
Many many thanks to Stephen Cohen and Bess Ho for the brand ID good karma...and to Mike McCabe for the necklace charm which became an Ink Wizard tattoo which became part of the Contagion story.
When Will the iPhone Allow External Biomed Sensor Integration? Don't Hold Your Breath...
“Unfortunately, the actual implementation of integrating a meter and the iPhone is a process filled with tribulations-mostly internal factors like budget reviews, business development, marketing, hiring of iPhone developers, legal counsel approval, and so on,” Tendler writes. “Everything moves very slowly at the large corporate level. Plus, external factors such as FDA regulations provide extreme liability for a company at this level.”
Read the entire column here.
| 7.16.09 | Qualcomm pulls the plug on LifeComm - Inbox - Yahoo! Mail
23.7.09
@jensmccabe - Exploring the 'Me-ome' 23a
More data, including the weighted-decision making matrix I used to decide to share my genomic data open-source style, coming soon!
99$. 23andMe's Research Revolution was *so* worth it...
Personal health action item 1: Ask doctor at appointment Friday about Celiac's Disease variant(I haz it! Shocker!).
21.7.09
Quantification of Self - Choice and Control Aware Care (Participatory Medicine Part II) Will REQUIRE IT
|
Health InfoViz? I Wish...Taking Notes From Emanio EDI Software

Where's my CONTEXTUAL dashboard for healthcare decision-making? http://www.emanio.com/Context/
2008: The Year of EMRs? Nope - The Year of Telemedicine
I am the CEO of a large physician network in CT.
There were four new CPT codes for 2008:
99441 PHONE E/M BY PHYS 5-10 MIN
99442 PHONE E/M BY PHYS 11-20 MIN
99443 PHONE E/M BY PHYS 21-30 MIN
99444 ONLINE E/M BY PHYSUnfortunately, in my state (CT) hardly any of the large healthplans will pay for these codes, even though Medicare pays for 99441-444 in 2009 ($15-$41). It is hard to get physicians to adopt new modes of patient care if they are forced to make large investments in technology with scant prospects for reimbursement for services utilizing this new technology. I guess we all must hope that the big EHR vendors will all provide free upgrades (dream on) to make sure their products can guarantee 'meaningful use" in 2011 so docs can receive some of their investment returned. I'm not holding my breath.
From "The Health Care Blog: The Doctor Is In and Logged On."
Perhaps by 2011 we'll finally get around to the Year of eHealth, and then by 2015 we may be approaching the mHealth era...that is, if our healthcare reform budget doesn't become the next financial system fiasco.
20.7.09
"We are all made of stars..."

Next time someone tells you you're glowing, thank them. Seriously.
Even more fascinating is that the light human subjects in the Japanese study emitted did NOT correspond to thermal imaging.
Take a look also at the 'third eye' (ajna chakra). It wouldn't be an out-there theory if I didn't tie it into genoanth somehow...brain stem develops as result of maternal or paternal chromosome?
Rockin' research link courtesy of @realmarcin.
Individual Reforms First - Saving Our Healthcare System Requires Healthier N=1 Decision-Making
Getting millions of people to go to a polling place on one specific day to pull a lever, touch a screen or mark a ballot using social media really isn’t all that complicated.
Using social media to get one obese 68-year-old man who lives alone to test his blood sugar three times a day for the rest of his life? Now that’s a social media challenge.
From Craig Stoltz's "Social Media, Health IT and Gov 2.0 | Web2.0h...Really?"
17.7.09
Corporate Fashion, Contagion Health Style

Yes, I have no fashion sense, unless Threadless is considered cutting-edge.
However, I have to admit I'm drooling over the near-blinding shade and design of this Attus Aparel CEO jumpsuit.
Would I be brave enough to sport this with Doc Maartens at a healthcare conference this fall? Hmmm....
From: "http://www.attusapparel.com/jumpsuits/"
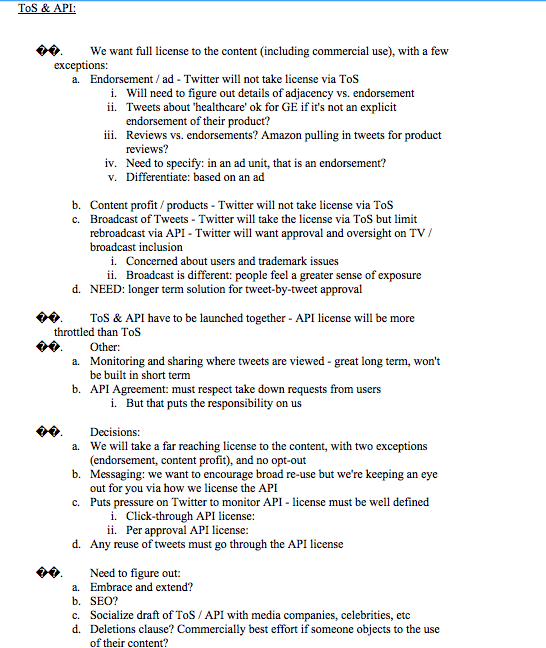
Has Twitter Been Chatting with GE? If You Thought Twitter Wasn't Paying Attention to Healthcare Content, IP - THINK AGAIN

From this TechCrunch coverage (amazing): http://www.techcrunch.com/2009/07/16/twitters-internal-strategy-laid-bare-to-be-the-pulse-of-the-planet/.
Thanks @garrytan for the heads up.
Health folks, take a look at item a, ii.:
"Tweets about 'healthcare' ok for GE if it's not an explicit endorsement of their product?"
Will I have to 'buy back' the IP for my tweets from Twitter at some point to prevent them from obtaining 'full license to the content?'
If that becomes the case, Twitter, I love you, but I will not stay in that sort of abusive relationship...
At the Forefront of Telehealth Implementation in...Ottawa?
The University of Ottawa Heart Institute cuts its hospital readmission rates 54% for patients participating in a home telehealth monitoring program. The program is also attributed with saving $20,000 for each patient not re-admitted.
From "HISTalk."
16.7.09
Got e-Prescriptions? Scotland Rolls out Electronic Acute Medication Service (eAMS)
Scotland has announced that it has become the first country in the UK to deliver an electronic prescription service, with more than 90% of prescriptions now submitted electronically.
Scottish health secretary Nicola Sturgeon said the electronic Acute Medication Service (eAMS) was the first national system of its kind to go live anywhere in the UK and was now enabled in 99% of Scottish GP practices and pharmacies.
The eAMS prints a barcode on prescriptions at a GP surgery and sends a message to Scotland’s ePharmacy Message Store.
When a patient presents at a pharmacy with their barcoded prescription, the pharmacist can scan the barcode to pull down the prescription and dispense the medicine.
Dispensing a prescription triggers the creation of an electronic claim message to NHS National Services Scotland (NSS).
The Scottish government said eAMS cuts the risk of errors between GPs and pharmacists, delivers improvements such as the use of universal codes for virtually all medicines, and boosts efficiency.
From "E-Health Insider Primary Care :: Scotland delivers e-prescription service."
Futurist or "Watcher" Thoughts on Healthcare Reform: "The Future I See Doesn't Look So Good..."
"...the good news is, the future is always changing. In the largest of ways, by the smallest of things. They've been winning a lot of battles, now it's our turn to win the war."
e-Patients. Remember, the time is now. But let's prevent war if we can. Olive branches folks, olive branches.
Quote from the 2009 movie "Push."
Video from: "The Trailer for Paul McGuigan's Push! - Superhero Hype!"
15.7.09
Diabetes itself doesn't up risk of depression | Health | Reuters
Although people with diabetes have a higher risk of being diagnosed with depression than other people, a large new study has found that much of that increase can be accounted for by their more frequent contacts with the medical system, rather than the diabetes itself.
But frequent contact with the medical system does?
Read the second graph in this article (link at bottom of graph above).
US Democrat Health Reform InfoViz - I Wish This Was a Joke...
| http://docs.house.gov/gopleader/House-Democrats-Health-Plan.pdf Hat tip to @oldbailey. Please note patients and providers are LITERALLY at opposite ends of the chart. Frightening. Jen S. McCabe @jensmccabe CEO/Founder: Contagion Health CoFounder: NextHealth (NL) Consulting/Chief Patient Advocate (social media): OrganizedWisdom Health LinkedIn: Jen McCabe Skype: jenmccabe iPhone: 301.904.5136 Dutch Mobile: +31655585351 jennifermccabegorman@yahoo.com |
What are PHR "Top 5" Features? NHS HealthSpace PHR Survey Asks Patients...(Paraphrased)
On page 3 of the HealthSpace survey, the NHS is asking patients to rate features the NHS "might be able to make available to people using HealthSpace." Patients are asked to select 'Top 5' features from the list and state how often they would use the Top 5 (daily, very regularly/weekly, quite regularly/monthly, infrequently/2-3x per year, never, don't know). In parenthesis, I've placed examples (not comprehensive by any means; feel free to make additions by leaving a comment) of US services or types of systems/documents that have these features, but are stored in a variety of different places under our current rabbit-warren of disconnected storage. Features listed include: Jen S. McCabe
Question: Which 'Top 5' features would you choose for a PHR (personal health record?) Is the list MISSING any features you'd consider top shelf? @jensmccabe CEO/Founder: Contagion Health CoFounder: NextHealth (NL) Consulting/Chief Patient Advocate (social media): OrganizedWisdom Health LinkedIn: Jen McCabe Skype: jenmccabe iPhone: 301.904.5136 Dutch Mobile: +31655585351 jennifermccabegorman@yahoo.com |
Imagine That - Ask Patients for Input on PHR Functionality (NHS HealthSpace)
Patients are being invited to give their views on the future development of the Department of Health’s personal health record project, HealthSpace.
An online survey asks patients to give their views on what functionality they would find useful and how often they would be likely to use such features.
The survey follows moves to shelve the planned expansion of HealthSpace, as revealed by EHI Primary Care last month.
An £80m plus business case had been prepared by NHS Connecting for Health, outlining plans to make HealthSpace a hub for transactional services.
Under the plan, patients would have been able to book nurse or GP appointments, manage long-term conditions, order repeat prescriptions or medication reviews and complete pre-registration assessments online.
However, the business case appears to have been kicked into the long grass by the DH and not submitted to the Treasury as originally envisaged.
Now, the survey is seeking patient views on these services. It asks patients to pick their top five features and to log how frequently they would be likely to user them.
It also asks patients what steps they would be prepared to take to register for enhanced functionality, including completing processes online or face to face at a GP surgery.
The survey has been emailed by health helpline NHS Direct to more than 11,000 patients and is available on a variety of health-related websites including NHS Choices, Age Concern, SAGA and National Voices, the umbrella group for national voluntary organisations representing users of health and social care in England.
The current HealthSpace functionality means anyone over age 16 can register for a HealthSpace account.
This enables them to log and monitor their personal health information, provides a search system for local NHS information and access to the Choose and Book online booking service.
Dr Gillian Braunold, clinical director for the Summary Care Record and HealthSpace, said: “By using HealthSpace patients can make sure they are able to exchange knowledge with those providing their care.
"In pilot sites, HealthSpace is enabling citizens to have access to their Summary Care Record and through the Communicator function have secure communication with NHS staff caring for them. Ultimately HealthSpace is all about putting patients in control of their health."
The survey is available until 17 July and CfH said the results would be analysed to help determine the future direction of the HealthSpace service
Read the article en toto.
Would love to hear if any UK/NHS Twitter users were involved in pilot/survey design or are using HealthSpace at a pilot site....
56% of Americans Using the Web for Health Info Say Search "Changed Their Overall Approach"
Of the 61% of Americans who use the internet for medical information, six-in-ten say they or someone they know has been helped by following health advice found online, up significantly from 2006 when only 31% of e-patients said this. Only 3% of e-patients say they or someone they know has been harmed by online health information. Among those searching the internet for medical information, 60% say what they found online in their most recent search affected a decision about how to treat an illness or condition. Majorities also say the search changed their overall approach to maintaining their own health or that of someone they care for (56%) and that it lead them to ask their doctor new questions (53%). Fewer e-patient's said their health search affected a decision about whether to see a doctor (38%) or changed how they coped with a chronic condition or managed pain (38%).
Daily Number: Search Health - Pew Research Center
14.7.09
Senator Grassley's -Ah-Unique Healthcare Spending Solution
From http://healthcareforamericanow.org/page/s/job: "Senator Grassley's health care solution? Get a job like his."
Good grief. Capitol Hill is completely out of touch.
Hilarious comeback by Healthcare For America Now, which provides a form letter for you to apply for a job with Senator Grassley:
WANT HEALTH CARE AS GOOD AS SENATOR GRASSLEY'S? APPLY FOR A JOB WITH THE FEDERAL GOVERNMENT!
Senator Grassley pays $356.59 per month for health care, and the most he pays when visiting a doctor or hospital is $300.1 Senator Grassley's health care bills are paid by you and me.
Will Senator Grassley vote for health care reform that gives your family coverage that’s as affordable as his? So far his answer is NO. Instead, Senator Grassley says you should get a job with the feds.
So, fill out your name below to apply for a job with Senator Grassley so you can get the same benefits he gets. We'll deliver your job application to his office so you can get the care you deserve.
Have to admit, I'm sorely tempted:
Senator Chuck Grassley
Attn: Human Resources Department
135 Hart Senate Office Building
Washington, DC 20510
To Whom It May Concern:
I really need good health care benefits. Senator Grassley says that I should come to work for the federal government, so I can get benefits like he has, that my family can afford. So please consider this letter a job application.
I work hard, and I pay my taxes, but I cannot keep up with health care costs that are rising four times faster than wages if I can even get health care at all, what with all the denials of needed care that my insurance company throws in my way. Meanwhile, Members of Congress get health care that’s affordable , and nobody is going to deny care to an elected official!
Senator Grassley has so graciously offered to provide me health care as good as he has if I work for the federal government, and so I am applying for a position in Senator Grassley's office in the hope he will make good on that promise. If he cannot, the only hope I have to obtain quality, affordable health care for me and my family is if Senator Grassley drops his opposition and supports real health care reform - reform that gives me a choice of public or private insurance, make care affordable, and delivers good benefits.
Maybe one day, I'll be able to have the same health care benefits Senators like Chuck Grassley have.
I look forward to your response,
[your name]
US Military Medicine Gets a New Cadet - Meet Sergeant Elmo
Elmo, the fire engine red Sesame Street Muppet, will make a special guest appearance with Army Brig. Gen. Loree Sutton, director of the Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury, at a press conference in Philadelphia next week. She will unveil how Elmo and his pals can help kids deal with the stress of military deployments.
Brig. Gen. Loree Sutton
This is part of a continuing outreach project with the Muppets that Sesame Street and the Defense Department kicked off in 2006, using familiar characters to help children in military families deal with tough challenges posed by both deployment and a parent's return home.

Well tickle me happy (couldn't help myself).
From "Elmo and the Brigadier General - What's Brewin.'"
12.7.09
Support Obamacare? What President Obama Wants From the American Public
Jen --
As we speak, key committees in Congress are weighing options and making final decisions about how to tackle health care reform. This could be one of the last opportunities to shape the legislation before it's written.
The behind-the-scenes committee negotiations aren't front-page news, but the lobbyists trying to block reform are following every detail, and they won't miss a day. If the final plan is to uphold President Obama's principles of reduced costs, guaranteed choice -- including the choice of a robust public insurance option -- and quality care for all, your voice must be heard.
Please write a short letter to the editor of your local paper expressing your support for President Obama's three principles for real health care reform, and asking your Congressional representatives to do the same. You can write and submit your letter in just a few minutes using our simple online tool.
These letters are an easy but powerful way to make a difference. The letters section is one of the most-read parts of the newspaper, and decision-makers in Congress and the media watch it closely to gauge where the public stands.
Good letters are usually just two or three short paragraphs. You can just explain that you're a local resident who knows we need real health care reform following the President's three principles, and we need it now. If you have a personal experience with the health care system that motivates you, that will make the letter even more powerful.
The opponents of real reform have deep pockets and insider access, and they're holding nothing back in their drive to derail progress before the plans go public.
Your letter, submitted at this time, can help remind your representatives that the American people are counting on them to stand up to special interests and deliver the comprehensive reform we so desperately need.
http://my.barackobama.com/healthcareletter
Thanks for all that you do,
Mitch
Mitch Stewart
Director
Organizing for America
P.S. -- These letters are a vital first step. Stay tuned for other critical ways to organize locally and make a difference in this campaign. We can only win this thing if we all work together every step of the way.
Paid for by Organizing for America, a project of the Democratic National Committee -- 430 South Capitol Street SE, Washington, D.C. 20003. This communication is not authorized by any candidate or candidate's committee.


1. Published support for generalities.
2. Money.
Grrrr.
From an email I received titled: "A critical time for health care reform."
President Obama (Mitch) - you are losing our support and the excitement you have successfully generated with 'grassroots' social media campaigns like individual emails, Twitter use, the ability to interact via web commentology, etc.
People who ask too often for my time and money (repeatedly) in mass-blast format are often removed from my list of contacts. I don't want to do this to your healthcare reform updates/emails, but you're leaving me few other options.
Your emails are currently viral, and not in a good way. Please please please take a closer look at your approach.
Health 2.0 Meets Government Stimulus - Network World
"Meaningful use" is the term that is written in the ARRA legislation to define investments eligible for reimbursement. More specifically the product or service must demonstrate use of a "qualified EHR" in a "meaningful manner." But this definition is not settled and the process for certification of these products and services as compliant with the definition is not final.
"This definition [meaningful use] will be a major factor in how innovative the EHR systems can be" said Vince Kuratis President of Better Health Technologies. "If it is too narrow the EHR systems that become eligible for subsidizations may lack leading edge interoperability with a limited capability to serve as a platform for new and transformative applications of the EHR data. This outcome would be the equivalent of manufacturing a 2002 Chevy Suburban for today's car market." Kuratis is one of a growing number of proponents of a multipurpose EHR that will empower patients to be their own advocates and as an EHR that serves doctors to improve a patient's healthcare. Further, anonymized EHRs can be elements of large data sets unidentifiable to any person, which can be analyzed to improve healthcare investments and support better epidemiological decisions. They want the definition to allow younger disruptive Health 2.0 companies that have novel applications of the EHR platforms to be eligible for generous amounts of the stimulus money.
Must read for anyone building an EMR, EHR, PHR platform.
From "Health 2.0 Meets Government Stimulus - Network World."
11.7.09
Benefits of Attending HackCamps Like SuperHappyDevHouse, Cupertino CA

| You sit, packed sardine/LAN-party style on tables, literally elbow-elbow with developers/engineers coding kick-a@$ stuff like Tweepsect (by @shazow). And get to watch them monitor hits and make requested updates in real-time. Rockin.' Jen S. McCabe @jensmccabe CEO/Founder: Contagion Health CoFounder: NextHealth (NL) Consulting/Chief Patient Advocate (social media): OrganizedWisdom Health LinkedIn: Jen McCabe Skype: jenmccabe iPhone: 301.904.5136 Dutch Mobile: +31655585351 jennifermccabegorman@yahoo.com |
10.7.09
We Are Eating Ourselves to Death, Personally and Economically
Healthcare spending on obese patients in the U.S. has ballooned, growing more than 80% over a five-year period, researchers have found.
From "Medical News: Obese Account for Greatest Jump in Healthcare Costs" - in Primary Care, Obesity, MedPage Today.
Actually, healthcare spending increases across the entire girth are frightening...to wit, the 25% increase in expenditures for 'normal-weight' patients.
7.7.09
Never Heard a Doctor Say That...
"I surprise my patients by asking, ‘Is there anything else you want to talk about today?’ They’ve never heard a doctor say that."
DR. HARRY J. SHRIVER 3d, chief of a clinic near Seattle run by a health insurance cooperative."
"Is there anything else you want to talk about today?" should not be a surprise question coming from your doc.
From the NYT e-newsletter edition-Quotation of the Day.
Open-Sourcing Patient-Driven Genomic Research with 23andMe's Research Revolution - Will it Work?
I've been laying in wait a long time-patiently-for my chance to be involved with the evolution of DTC genomics and public/personal health research in a way that makes sense.
Moving to San Francisco, devouring GenomeWeb daily - all of these have been precursors for the advocacy role I'm embracing from here on out.
Today I'm participating in the FIRST patient-driven genomic research campaign. Today the 23andMe Research Revolution begins.
(The lovely video of me spitting comes direct to your browser from YouTube. Warning: Footage contains moments of extreme viscosity. Don't say I didn't warn you).
If you haven't had the spit-kit, DTC genomics experience, 23andMe is giving you a unique chance to give up some saliva for a decent cause, and pretty much the only one I'm working for these days - patient-driven research and self-advocacy.
I'll be very blunt about why and how I'm cheerleading the Research Revolution cause. If first-person narrative form makes you feel squirmy and twitchy, put your perusal of my blog(s) and tweets on hiatus until this fall.
I'm going to be sharing a lot of details, blunt-force-trauma style, about why I'm choosing to do things like spit in a tube, champion consumer access to genomic data, and participate in screening and pre-evaluation process for the Personal Genome Project. If accepted, I'll open-source my genome. Here's why I'd be crazy enough to do something like that...
If you read my blog and/or tweetstream, you know I'm:
1. Fanatically devoted to establishing patient-centric, n=1, individual first-exponential second, modalities of research and care delivery.
2. Near obsessed with the DTC genomics market - after all, it's the only place where my health data is REALLY #myhealthdata. My spit, my kit, my results. I think 23andMe is providing a model for access and ownership of personal health information as MY asset that the rest of the system will be dragged into adopting, kicking and screaming.
3. Scared near-witless about intellectual property laws and genetics, aka the ability of corporations (like Myriad) and/or organizations (or even individuals) to patent genes. I can't stomach the possibility that in the future I won't have access to the most intimate coding of my personal composition - my genetic data - and will do everything I can to advocate against genomic slavery now. It's a radical stance, yes, and I hope we all look back on this post 8 years from now, term me the "girl who cried wolf" and laugh. I'm afraid we won't. I'm afraid someone else will someday hold the rights to modify/share my genetic info, and I'll be blocked from accessing or 'donating' it to public research efforts like this one at will. I can't sit idly by and wait for that to happen.
You'll see many more eloquent updates in the coming weeks as I go on the genetic testing journey of self-discovery, self aggrandizement, and self-doubt, but for now I'll keep it to the 'ask.'
And it's actually a selfish, not a selfless, one.
I need 23andMe to make this model work for one or more of the first 10 'test' conditions so we can get around to researching a disease that hits below me the belt both personally and professionally - bipolar disorder.
Here's the deal.
We need 1k - 2k participants PER CONDITION to prove that this 'open-source' patient-driven research thing really works.
We need those kinds of big eye-popping numbers to take to foundations, and grant-makers, and government orgs, and universities, and research institutions who are doing the latest and greatest in condition-specific research.
These kind of people need some proof of the hard number variety, not just a puffed up sense of importance that comes from nice comments on a Facebook page, or thousands of follower on Twitter (gulp) or photos of the spit kit experience (fun as it is to document - it felt like configuring a personal chromosomal time capsule).
Here's the kicker.
Disease research is expensive, no matter who you are, and how much money you've got. I don't have a lot, but I'm going to be giving Chia Hwu, 23andMe's Community Manager and one of the Research Revolution gurus wrangling this program, her first $99 Research Revolution check tomorrow.
I could have gotten my spit kit for free, but I decided this afternoon I'm committed to going through the process like every other advocate and community leader who signs on to champion this kind of research evolution.
Here's the thing: We need to prove the power of patients to self-organize so we can go after subsidies and grants for this type of research. That means us early adopters, as so often happens, will have to pay up front to get things started - $99 in this case. Trust me, I pushed on this.
I wish 23andMe could offer this first round of research for free. My personal goal is to help prove a model that one day provides complete subsidization of genomic research for those who are willing to 'donate' DNA. Donating genetic material for public health research will, one day, be as systematic as donating some platelets during a blood drive. Maybe we'll even get donuts afterwards.
I'm hopeful we'll see partnerships with companies sponsoring employee involvement, foundations giving matching grants to support condition-specific community growth, etc. in the near future, but we've got to make one hell of a strong case first. We need to show individuals are willing to step up and self-organize.
Can we do it? I honestly don't know. But I think if people-who-are-patients want to storm the ivory tower of research that is academically and/or economically driven, we've got to start here. We've got to try.
But to make that work, we've got to make this work first. I'll be working with 23andMe to help find champions for these initial 'test case' conditions. As fast as I can, because, as I said, I've got a family of bipolar patients (literally and figuratively) whom I'm committed to protecting, to defending, and to advocating for lives with better, more personalized treatment modalities.
If it helps cure, or even develop better treatments for bipolar disorder, I'll open-source my entire genome, as soon as I can swing the sequencing. I've known too many people who've lost years, given up hopes, and sacrificed possibilities on the bloody altar of this condition. I won't be one of them.
So about that ask...What do I want from you? It's pretty simple. I want you to join, one way or another.
Comment. Get involved. Blog about Research Revolution. Keep talking about #myhealthdata, and where you feel like you own it (or not).
Ping me on Twitter (@jensmccabe, @polarwisdom), or get in touch with Chia (@23andMe, @chiah).
Revolutions are just the type of movement I like to see getting started.
To help get this one off the ground, I'm putting my $ where my mouth is...
I'll personally pledge a matching gift to support 2+3 captains and advocates (5 total this first round) for the Research Revolution program.
Leave a comment here with your country of residence/citizenship (has to be in one of the 23andMe 'ship to' countries) and which of the ten 'ground zero' conditions you'd like to advocate for, and WHY.
You've got 2+3 days (5) to submit.
I'm tired of talking about getting involved, preaching about what we can do differently, and sitting around at HealthCamps b*&tching about why nothing is changing.
I'm offering up chromosomes to make a difference. What have you done for health reform lately?
UK Closer to #myhealthdata? Allows Patient Choice in Transferring Records to Private PHR Firms?
NHS records could be transferred to private companies under plans being drawn up for the Tories.
The party has commissioned a review of the sprawling NHS computer system that may conclude patients should instead be given the option of moving their data to firms such as Bupa, or even Google or Microsoft.
Privacy concerns over Tory plans to farm NHS records out to private firms | Mail Online
Fascinating. Keep an eye on the NHS debate about allowing patients the option to move data to private PHR offerings.
By Finesse or By Force? How Will the Patient-Centric Revolution Advance?
Patients are going to have to force themselves into this debate against the resistance and indifference of the Washington establishment. Patients cannot afford the luxury of deference and e-mail.
Craig Stoltz: Washington Post's "Salon" Disaster and Health Care Reform
Agree? Disagree?
3.7.09
Biggest Issue for Next-Gen Gene Sequencing = Where Do We Store Data?
What's the biggest limitation to next-gen sequencing?GenomeWeb Weekly poll
18% Library preparation
17% Read length
13% Multiplexing
45% Data storage/analysis
5% What limitation? It's a perfect process already.
Audience/reader poll results from GenomeWeb's daily newsletter. These results are from last week's poll.
More Dangerous Than Swine Flu - Your Lunch++++
..."Not a single state posted a decrease in obesity, and three of every ten children living in 30 states are overweight or obese, said Jeff Levi, PhD, executive director of the Trust for America's Health, which compiled the "F as in Fat" report with the Robert Wood Johnson Foundation.
Overall, two-thirds of Americans are either overweight or obese, the report found.
Americans' access to healthcare, the $ costs of healthcare reform, swine flu colonizing the world over - all of these are far less frightening than the fact that we are greedily committing suicide-by-caloric-intake.
We are, quite literally, eating ourselves to death.
Before you read the coverage, fix your gaze on this beauty of a closing sentence:
"By way of contrast, in 1991, no state had an obesity rate above 20%."
In less than 2 decades, states obesity rates continue to rise by 1+% PER YEAR and NOT A SINGLE STATE posted a decrease in obesity rates over the past year.
Forget outsourcing. Forget the innovation economy. Forget fixing science/math education. If we don't focus on fixing obesity NOW, in 3 more decades there won't be enough of a workforce left to worry about the economic viability of this federation of states.
More really scary stuff from Medpage coverage of the Robert Wood Johnson Foundation's frightening "F as in Fat" report:
"Sixteen states experienced an increase in obesity rates for the second year in a row, and 11 states experienced an increase for the third straight year.
Moreover, America's vast waistline is "a big contributor to the skyrocketing healthcare costs in the U.S. How are we going to compete with the rest of the world if our economy and workforce are weighed down by bad health?" Dr. Levi asked.
Mississippi was once again the fattest state with 32.5% of it adult residents obese. But Mississippi was not an anomaly in the region -- eight of the top ten states are in the South.
Here are the report's top 10-ranked by percent of obese adults:
Mississippi (32.5%)
Alabama (31.2%)
West Virginia (31.1%)
Tennessee (30.2%)
South Carolina (29.7%)
Oklahoma (29.5%)
Kentucky (29.0%)
Louisiana (28.9%)
Michigan (28.8%)
(tie) Arkansas (28.6%) and Ohio (28.6%)
According to the report, adult obesity rates now exceed 25% in 31 states and exceed 20% in 49 states and Washington, D.C."
Calling All Non-Scientists...
"Principles of Open Source software did not prove to be useful in open drug development. ... Crowdsourcing will not advance quantum physics," he writes. "Open Science in its fullest form is not an issue that scientists can truly solve by themselves."
Open Science's Greatest Need Is ... Non-Scientists? | The Daily Scan | GenomeWeb
Please read the great post examining models of 'open science by Pawel.
While I agree with much of the chewy content goodness, I'm not sure I can sign on to the bit about 'principles of open source software did not prove to be useful in open drug development' being entirely true.
The capability for open source to be useful in things like crowdsourcing new theories of genetics+anthropology (genoanth) in addition to drug development hasn't been proven, but it certainly hasn't been disproven.
Especially in health analytics/personal biometrics ("Me-trics" or the #quantifiedself) Joe the Plumber hasn't had access to the kind of data about ourselves (much less others) that we'd need to share and contribute to an open-source public health development initiative.
Cancer-survivor communities like ACOR (@gfry, @ePatientDave thanks again for the heads up here) COULD in theory be used to open-source new treatments. In fact, the community/listserv members ARE using the list this way, but the 'establishment' isn't paying much attention.
PatientsLikeMe.com, however, has made open-sourcing one's health data relatively easier, lowering barriers to entry by putting metric tracking/analytics tools in the hands of patients.
Despite my fan-girl-ism for PLM, there are issues with the service, which isn't 'pure' opensource (in my opinion) - I cannot opt out of having my data anonymized and sold, and I can't demarcate if it's used for corporate gain versus nonprofit research purposes. I also can't throw my data open for the world to use/view at will if I so choose.
If I was designing an open-science, open-source health development initiative (product or drug), I'd go after a software installlation like that offered by Palantir Tech. Then I'd recruit survivors and start sharing data nodes. Then I'd motivate the community to go to work analyzing the hell out of the data intersection points for sparks of potential relevance. Then each promising x+y would have to be examined for causation/correlation.
If I wanted to cure a disease like Parkinson's, or even come up with EBP support (and EBP here would really be E2BP, for Evidence-based practice+ Experiential-based practice) for a new clinical guideline to impregnate into real-world practice, this is how I'd go about it.
I digress. But Pawel Szczesny (Freelancing Science) is right about one very big issue here - open science (or open source, or open health) absolutely require participation outside traditional professional gradients to succeed.
Talent without a pedigree counts for something here. Let's make sure we don't continue to make the mistake of discounting the value of experiential knowledge, which is open science (and 'open health's) most underutilized asset.





{kind=link}